Defining lung recruitability is needed for a safe positive end-expiratory pressure (PEEP) selection in mechanically ventilated patients with acute respiratory failure. However, no simple bedside method is available for identifying patients who may benefit (recruitment) vs. incur harm (hyperinflation) by various levels of PEEP and for indicating the potential advantage of recruitment as well as the risks of overdistension.
Electrical impedance tomography (EIT) is gaining popularity as a bedside non-invasive, radiation-free lung imaging tool that can continuously and in real-time visualize the ventilation distribution and lung volume changes. It is therefore a promising technology to monitor the potential impact of PEEP on determinants of ventilator-induced lung injury. EIT allows direct visualization of both the relative collapse and overdistension at different PEEP levels, but standardized methods for assessing recruitability and personalized PEEP selection with EIT are topic of ongoing discussion.
Therefore, in early 2020, the PLUG working group initiated the RECRUIT study: Lung RecruitmEnt assessed by eleCtRical Impedance Tomography (NCT04460859). This is an ongoing international observational study in patients with moderate-severe ARDS, with the main aim to verify the feasibility of measuring the potential for lung recruitment by EIT.
While the main study is still ongoing, the analysis of 108 ventilated COVID-19 patients was recently published: https://www.atsjournals.org/doi/10.1164/rccm.202212-2300OC. To date, this is the largest study in COVID-19 ARDS that presents a comprehensive EIT analysis and physiological assessment over a wide range of PEEP levels that was well tolerated by all patients.
PEEP maneuvers and recruitability
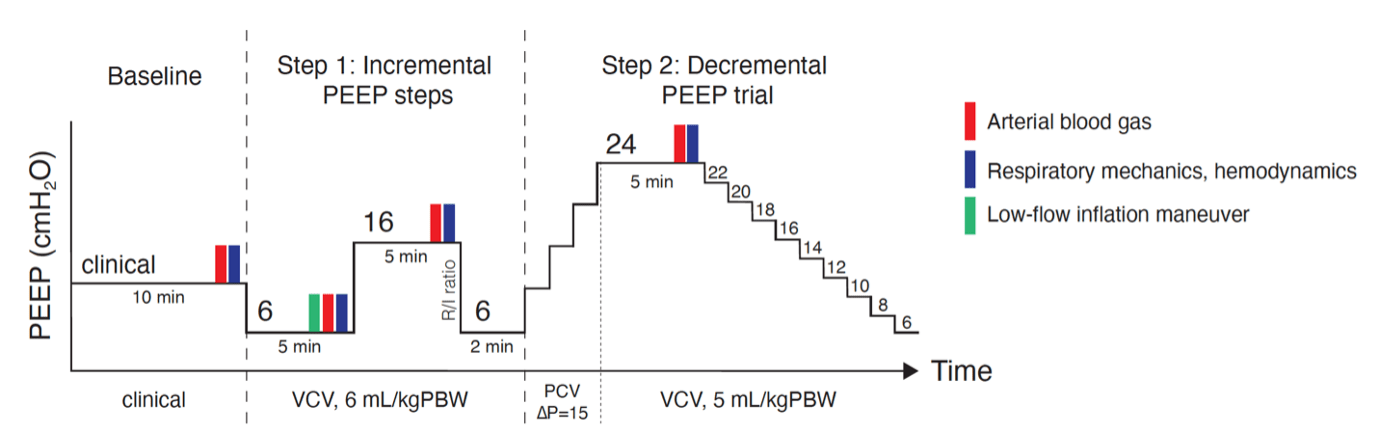
Various PEEP titration maneuvers were performed, including a 5-minutes PEEP steps of 6, 16 and 24 cmH2O, and thereafter a decremental PEEP trial from 24 to 6 cmH2O:

Considering that EIT parameters are derived from the calculus of relative changes in pixel compliance, we defined recruitability over the full range of PEEP levels that were applied. We defined recruitability as the amount of modifiable collapse when increasing PEEP from 6 (start of protocol) to 24 cmH2O (=ΔCollapse24-6). Patients were classified as low, medium or high recruiters based on the tertiles of ΔCollapse24-6, and we found that recruitability varied between 0.3% to 66.9%.
EIT-based optimal PEEP
The PEEP value at the crossing point of the collapse and overdistension curves obtained with a decremental PEEP trial indicates the level where collapse and overdistension are jointly minimized. This crossing point varied widely between the recruitability groups.

Interestingly, this EIT-based PEEP was associated with comparable respiratory mechanics across all degrees of recruitability: respiratory system compliance, driving pressure and normalized elastance were comparable between groups, and groups showed low levels of overdistention (<10%) and collapse (<5%) at this crossing point PEEP level. This means that, independent of the amount of recruitability, the crossing point PEEP could provide a PEEP level with good compromise between distension and recruitment.
EIT-based PEEP vs. Compliance-based PEEP
Individualized PEEP setting using the highest respiratory system compliance during a PEEP trial has been proposed and looks attractive since it can also yield the lowest driving pressure. However, we demonstrated that the crossing point PEEP does not match the PEEP related to the highest compliance in 81% of patients despite a correlation between the two methods.

These results stress that the overall compliance can poorly reflect the regional mechanics in different parts of the lungs. EIT can inform when (regional) distention is excessive, thereby avoiding to lose the potential benefit of recruitment.
Conclusion
Based on these results, we concluded that EIT is feasible for assessing recruitability and to support setting a personalized PEEP according to the best compromise between distension and recruitment. The impact of this approach on clinical outcomes has to be studied.
Next steps
The ongoing RECRUIT study is currently enrolling non-COVID-19 patients, until the final sample size of 171 patients is met. This will allow a next set of analyses on the correlation between recruitability and outcome, on the comparison of recruitability in COVID-19 vs. all-cause ARDS and on different methods to select personalized PEEP by EIT, plus many more exciting analyses that we could conduct on this extensive EIT database.
A special thank you to Annemijn H. Jonkman for this post.
Wonderfull! Is it possible to participate in This phase of the study?
In that case would be Great to get the info
Thank you
The contact information can be found on the Clinical Trials page. https://www.clinicaltrials.gov/study/NCT04460859
WHY DON´T WE TAKE INTO ACCOUNT THE BEST COMPLIANCE LINKED TO THE BEST DRIVING PRESSURE AFTER A RECRUITMEN MANEUVER AND DURING THE PEEP TAPERING PHASE?
INTHE RECRUIT STUDY, AS WELL IS AN OTHERS, A BETTER CLINICAL APROXIMATION OF THE BEST COMPLIANCE AND THE LOWER DRING PRESSURE HAS BEEN SHOW FOR THOSE CENTERS THAT DO NOT HAVE EIT.
THANKS